Medical marijuana is legally available to only nine people nationwide. The Compassionate Investigational New Drug (IND) program which supplies government marijuana to those nine is jointly administered by the Department of Health & Human Services (HHS), the National Institute of Drug Abuse (NIDA) and the Public Health Service (PHS)—which shut down expansion of the program two years ago, claiming that it sent a “bad signal” to the American public. But with the arrival of the Clinton team in Washington, more tolerant winds may be blowing through the corridors of power. Following an order from Secretary of Health Donna Shalala to review the Compassionate IND, rumors have been dying that the program will be opened to new applicants any day.
PHS spokesman Bill Grigg confirmed that meetings regarding the program have occurred—but said they concerned “how to proceed to look at the issue, rather than on whether and when to reopen the program.”
If the Administration does decide to reopen the program, it faces a road riddled with political and bureaucratic land mines. Keeping it shut is similarly unacceptable: people are going blind from glaucoma and suffering needlessly from the “wasting syndrome” associated with AIDS, muscular disorders, and side effects from cancer chemotherapy. Which way will the Administration turn? Difficult to say. But the story of the creation and closure of the Compassionate IND program must be looked at to grasp what is at stake.
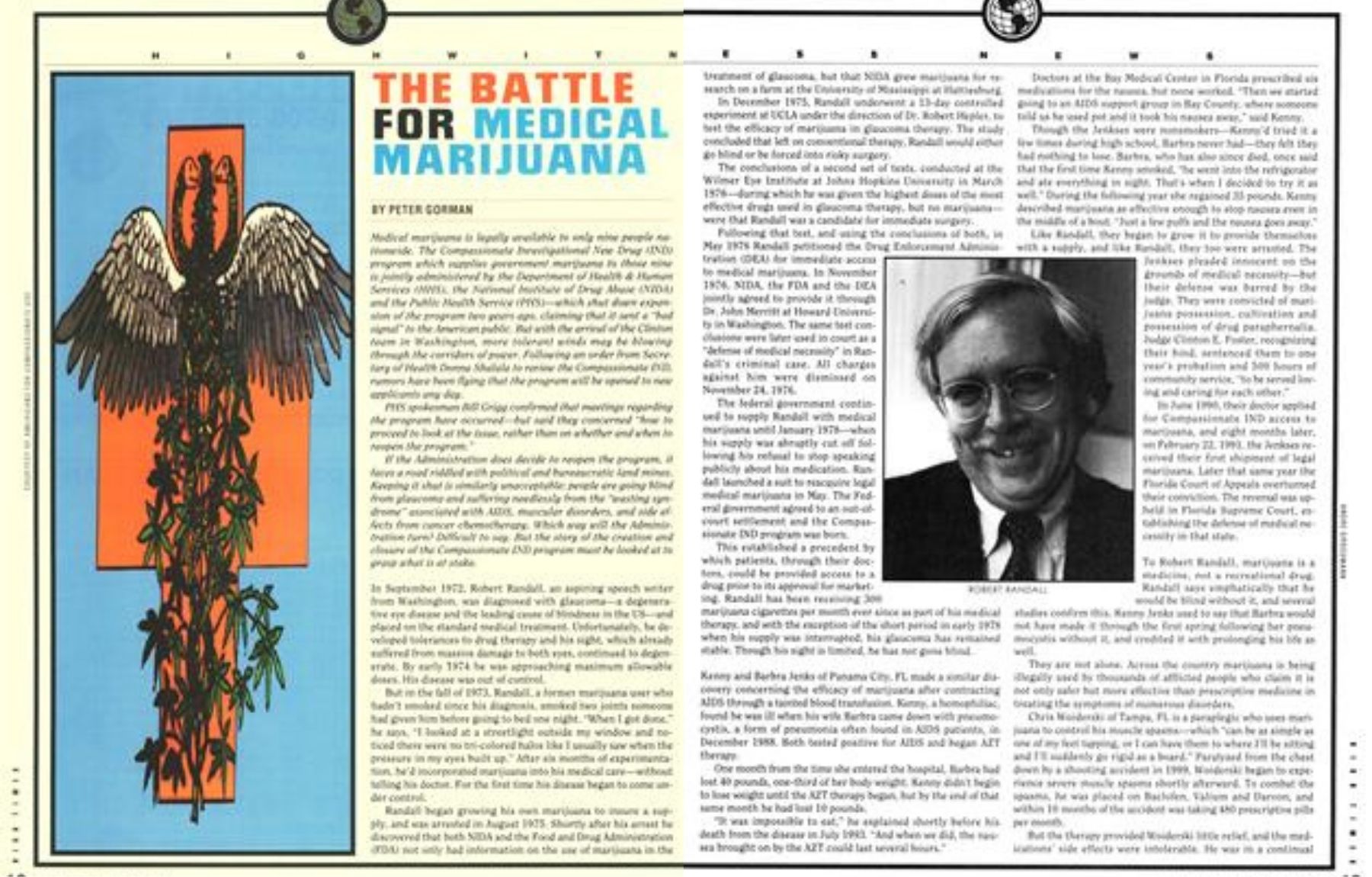
In September 1972, Robert Randall, an aspiring speech writer from Washington, was diagnosed with glaucoma—a degenerative eye disease and the leading cause of blindness in the US—and placed on the standard medical treatment. Unfortunately, he developed tolerances to drug therapy and his sight, which already suffered from massive damage to both eyes, continued to degenerate. By early 1974 he was approaching maximum allowable doses. His disease was out of control.
But in the fall of 1973, Randall, a former marijuana user who hadn’t smoked since his diagnosis, smoked two joints someone had given him before going to bed one night. “When I got done,” he says, “I looked at a streetlight outside my window and noticed there were no tri-colored halos like I usually saw when the pressure in my eyes built up.” After six months of experimentation, he’d incorporated marijuana into his medical care—without telling his doctor. For the first time his disease began to come under control.
Randall began growing his own marijuana to insure a supply, and was arrested in August 1975. Shortly after his arrest he discovered that both NIDA and the Food and Drug Administration (FDA) not only had information on the use of marijuana in the treatment of glaucoma, but that NIDA grew marijuana for research on a farm at the University of Mississippi at Hattiesburg.
In December 1975, Randall underwent a 13-day controlled experiment at UCLA under the direction of Dr. Robert Hepler, to test the efficacy of marijuana in glaucoma therapy. The study concluded that left on conventional therapy, Randall would either go blind or be forced into risky surgery.
The conclusions of a second set of tests, conducted at the Wilmer Eye Institute at Johns Hopkins University in March 1976—during which he was given the highest doses of the most effective drugs used in glaucoma therapy, but no marijuana— were that Randall was a candidate for immediate surgery.
Following that test, and using the conclusions of both, in May 1976, Randall petitioned the Drug Enforcement Administration (DEA) for immediate access to medical marijuana. In November 1976, NIDA, the FDA, and the DEA jointly agreed to provide it through Dr. John Merritt at Howard University in Washington. The same test conclusions were later used in court as a “defense of medical necessity” in Randall’s criminal case. All charges against him were dismissed on November 24, 1976.
The federal government continued to supply Randall with medical marijuana until January 1978—when his supply was abruptly cut off following his refusal to stop speaking publicly about his medication. Randall launched a suit to reacquire legal medical marijuana in May. The Federal government agreed to an out-of-court settlement, and the Compassionate IND program was born.
This established a precedent by which patients, through their doctors, could be provided access to a drug prior to its approval for marketing. Randall has been receiving 300 marijuana cigarettes per month ever since as part of his medical therapy, and with the exception of the short period in early 1978 when his supply was interrupted, his glaucoma has remained stable. Though his sight is limited, he has not gone blind.
Kenny and Barbra Jenks of Panama City, FL, made a similar discovery concerning the efficacy of marijuana after contracting AIDS through a tainted blood transfusion. Kenny, a hemophiliac, found he was ill when his wife Barbra came down with pneumocystis, a form of pneumonia often found in AIDS patients, in December 1988. Both tested positive for AIDS and began AZT therapy.
One month from the time she entered the hospital, Barbra had lost 40 pounds, one-third of her body weight. Kenny didn’t begin to lose weight until the AZT therapy began, but by the end of that same month he had lost 10 pounds.
“It was impossible to eat,” he explained shortly before his death from the disease in July 1993. “And when we did, the nausea brought on by the AZT could last several hours.”
Doctors at the Bay Medical Center in Florida prescribed six medications for the nausea, but none worked. “Then we started going to an AIDS support group in Bay County, where someone told us he used pot and it took his nausea away,” said Kenny.
Though the Jenkses were nonsmokers—Kenny’d tried it a few times during high school, Barbra never had—they felt they had nothing to lose. Barbra, who has also since died, once said that the first time Kenny smoked, “he went into the refrigerator and ate everything in sight. That’s when I decided to try it as well.” During the following year she regained 35 pounds. Kenny described marijuana as effective enough to stop nausea even in the middle of a bout. “Just a few puffs and the nausea goes away.”
Like Randall, they began to grow it to provide themselves with a supply, and like Randall, they too were arrested. The Jenkses pleaded innocent on the grounds of medical necessity—but their defense was barred by the judge. They were convicted of marijuana possession, cultivation, and possession of drug paraphernalia. Judge Clinton E. Foster, recognizing their bind, sentenced them to one year’s probation and 500 hours of community service, “to be served loving and caring for each other.”
In June 1990, their doctor applied for Compassionate IND access to marijuana, and eight months later, on February 22, 1991, the Jenkses received their first shipment of legal marijuana. Later that same year the Florida Court of Appeals overturned their conviction. The reversal was upheld in Florida Supreme Court, establishing the defense of medical necessity in that state.
To Robert Randall, marijuana is a medicine, not a recreational drug. Randall says emphatically that he would be blind without it, and several studies confirm this. Kenny Jenks used to say that Barbra would not have made it through the first spring following her pneumocystis without it, and credited it with prolonging his life as well.
They are not alone. Across the country marijuana is being illegally used by thousands of afflicted people who claim it is not only safer but more effective than prescriptive medicine in treating the symptoms of numerous disorders.
Chris Woiderski of Tampa, FL is a paraplegic who uses marijuana to control his muscle spasms—which “can be as simple as one of my feet tapping, or I can have them to where I’ll be sitting and I’ll suddenly go rigid as a board.” Paralyzed from the chest down by a shooting accident in 1989, Woiderski began to experience severe muscle spasms shortly afterward. To combat the spasms, he was placed on Baclofen, Valium and Darvon, and within 10 months of the accident was taking 480 prescriptive pills per month.
But the therapy provided Woiderski little relief, and the medications’ side effects were intolerable. He was in a continual drugged state which left him incapacitated. He suffered weight loss, insomnia, severe headaches and developed a problem with his left kidney that now requires surgery.
But while undergoing treatment at the Tampa VA hospital, several paralyzed vets told Woiderski they used marijuana to control their muscle spasms. “I’d smoked occasionally, but never since the accident,” he says, “and I was skeptical. So I investigated at the local university’s medical library and found several papers dealing with marijuana’s success with spasms. So I tried it.”
He discovered that half a joint in the morning before his first transfer from bed to the wheelchair controls his spasms for about six hours. Another half a joint during the afternoon controls them for the remainder of the day, and a whole joint before bed “lets me sleep without being tossed around all night.”
Since then, Woiderski has stopped all prescriptive medication, returned to college, and helped organize Paralyzed Americans for Legal Medical Marijuana (PALM).
On November 16, 1990, Woiderski’s neurologist—who wishes to remain anonymous—applied for Compassionate IND access to marijuana. He was approved on February 16, 1991, but has never received a shipment. HHS started to phase out the Compassionate IND program in June 1991, suspending all shipments to 28 recent approvals. On March 4, 1992, the program was officially shut down for all but those 13 persons who were already receiving the government pot. The only official comment made at the time of the program’s suspension came from PHS Director Dr. James Mason. “If it’s perceived that the Public Health Service is going around giving marijuana to folks, there would be a perception that this stuff can’t be so bad,” Mason told the Washington Post on June 22, 1991. “It gives a bad signal.”
Others in the Bush administration disagreed. Shortly before Mason made his comments, Herbert D. Kleber, the deputy national drug control policy director at the Drug Czar’s office, was “touting the program on national television as a ‘compassionate’ option that was available to seriously ill patients,” according to the Washington Post report. On January 31, 1992, the Los Angeles Times reported that Ingrid Kolb, acting deputy director of the Office of Demand Reduction, another post under the Drug Czardom, “said that dozens of patients who would have been eligible for the drug ‘are suffering from great pain— many are dying.’” She recommended that marijuana be given immediately to patients approved for it.
The decision to shut down the Compassionate IND program has placed thousands of medical marijuana users in the position of having to either continue to secure their marijuana illegally or forego the therapy altogether. “I resent being criminalized because the medicine I use for an incurable disease has arbitrarily been made illegal,” says Connie Tillman, an award-winning public-access cable talk-show host, the mother of two and a multiple sclerosis sufferer who says marijuana markedly decreases her muscle spasms. Others, like Fred Cole, agree. Cole, a fishing guide from Washington state, uses marijuana for back spasms resulting from a logging injury and has spent time in jail for growing marijuana for personal medicinal use.
Before the IND program was shut down, the government had implicitly acknowledged marijuana’s utility in treatment of glaucoma, chemotherapy nausea, chronic pain, the AIDS wasting syndrome and spasm disorders. But studies and anecdotal evidence also suggest it is beneficial in treating arthritis, anorexia, head injuries, epilepsy, migraines, PMS, sickle cell anemia, and stress disorders.
But if marijuana is so effective in the symptomatic treatment of these ailments, why is it illegal as a medicine? And why was the IND program shut down?
Marijuana had been popular in a variety of tinctures until the Marijuana Tax Act of 1937 made prescriptive use of the plant obsolete. The 1937 Act was opposed by the American Medical Association’s lobbyist, Dr. William C. Woodward, but the medical industry ultimately acquiesced to the new order.
There were few protests when the 1970 Federal Controlled Substances Act placed marijuana in the Schedule I category, meaning it had no recognized medical value or applications, and could not be used even for experimental purposes.
Shortly after the Compassionate IND program was shut down, Rayford Kytle, a PHS spokesman, was quoted in the April 1, 1992 Journal of the National Cancer Institute as saying that the program was closed because the “National Institute of Health believes there are better and safer treatments than smoked marijuana for controlling chemotherapy-induced nausea, relieving eye pressure caused by glaucoma and stimulating the appetites of patients with HIV-wasting syndrome.” Kytle added that NIH scientists believe the presence of carcinogens in marijuana smoke poses a significant health hazard to AIDS and chemotherapy patients, whose immune systems are impaired. “There was concern that NIDA’s supply could not keep pace with the increasing demand,” said Kytle.
Both Kytle and PHS chief James Mason made it clear that dronabinol—a synthetic derivative of marijuana, marketed under the name Marinol—would continue to be available for chemotherapy-related nausea.
While there have been no reliable reports of marijuana smokers who do not also smoke cigarettes developing either emphysema or lung cancer, studies indicate that heavy cannabis smoking does produce some respiratory system damage. If an alternate method of delivery could be devised— aerosol spray or vaporization are frequently touted possibilities—that damage could be eliminated. But current US laws banning the production of drug paraphernalia prevent experimentation with these methods. And until new delivery systems are available, proponents feel the potential benefits of smoked marijuana outweigh the dangers. They point to more than 2,000 years of historical medicinal marijuana use worldwide with no long-term negative effects.
Many doctors agree. In a 1990 study conducted by researchers Richard Doblin and Dr. Mark Kleiman, a random, anonymous sampling of 2,430 cancer specialists from the American Society for Clinical Oncology showed 48 percent of the respondents answering that they would prescribe marijuana if it were available, and 44 percent admitted they had already recommended illegal marijuana use to at least one patient.
Kytle’s concern over marijuana’s effects on the immune system also appears unfounded. While early studies did indicate that exposure to large amounts of cannabinoids produced alterations in the immune function of lab animals and cells in vitro, no studies on humans confirmed any correlation between marijuana use and impairment of the immune function.
Kytle’s third reason for the program’s closure, concern that federal supply would not keep pace with increasing demand, might be a reason for producing a larger supply—but doesn’t warrant additional comment.
As for Marinol, it is a synthetic form of the primary active constituent of marijuana, delta-9-tetrahydracannabinol, or THC.
While some users find relief through this pill form of THC, many complain that it doesn’t work as well as marijuana, that it takes longer to begin working, and that they prefer the dosage control they have when smoking marijuana. The National Cancer Institute agreed in a 1992 factsheet titled Marijuana for Chemotherapy-Induced Nausea and Vomiting: “Research has shown that the active ingredient THC is more readily and quickly absorbed from marijuana smoke than from an oral preparation of the substance.”
Medical marijuana proponents maintain that those suffering diseases for which there are no acceptable medical alternatives should have their therapy in the hands of physicians rather than the DEA, which controls the Controlled Substances schedule.
Despite the Public Health Service’s refusal to restore the Compassionate IND program, there is increasing evidence of a change in the public’s view of marijuana as medicine. Proposition P, a medical marijuana measure, was put on the ballot in San Francisco in 1991. It passed with an overwhelming 80 percent of the vote. And in 1992, in considerably more conservative Santa Cruz County, a similar ballot initiative gained 77 percent of the vote. Since then, dozens of similar initiatives and propositions have been passed nationally. Additionally, 35 states have endorsed the use of medical marijuana—although none of them are actually distributing cannabis at this time because the federal agencies which control the supply will not provide it. During the early ’80s, state programs in California, Georgia, Michigan, New Mexico, New York and Tennessee provided nearly 800 patients medical marijuana supplied by the National Institute of Drug Abuse, but federal bureaucratic interference and expense led to their closing.
This change in the perception of marijuana as medicine is rooted in a decision by the DEA’s own Administrative Law Judge Francis L. Young, who ruled in the case of Alliance for Cannabis Therapeutics, et al, vs. US Drug Enforcement Administration, in the matter of Marijuana Medical Rescheduling Petition. In his September 1988 determination, Judge Young said: “One must reasonably conclude that there is accepted safety for use of marijuana under medical supervision. To conclude otherwise…would be unreasonable, arbitrary and capricious….”
On the question of whether the marijuana plant, as opposed to synthetics such as Marinol, should be used, Judge Young said: “The cannabis plant considered as a whole has a currently accepted medical use in treatment in the United States…and it may lawfully be transferred from Schedule I to Schedule II.” The rescheduling would have legalized medical marijuana. But the DEA, under the direction of John C. Lawn, refused to act on Judge Young’s decision.
One of the consequences of the DEA’s refusal to reschedule marijuana was that many physicians who accept marijuana’s therapeutic value began to publicly call for the right to prescribe it. On March 17, 1992, the 450-member House of Delegates of the California Medical Association voted to adopt a resolution sponsored by Berkeley psychiatrist Dr. Todd Mikuriya which, while opposing the recreational use of marijuana, stated that “the therapeutic use of cannabinoids…may be appropriate for certain conditions.” More recently, the House of Delegates for the American Medical Student Association, at their 1993 Miami conference, unanimously endorsed marijuana’s rescheduling. And this past August 26, California became the fourth state to pass a resolution urging the White House and Congress to make marijuana prescriptively available.
These changes in public awareness of medical marijuana have been reflected in court decisions as well. In October 1993, a jury acquitted 39-year-old AIDS sufferer Sam Skipper of two counts of felony marijuana cultivation despite his admission that the more than 20 plants found in his California home were his. It was the first such acquittal in US history.
Additionally, the courts have recently taken a more lenient view of caregivers—those who provide marijuana to seriously ill patients. “Brownie” Mary Rathbun, a 70-year-old from San Francisco, was arrested in July 1992 when she was caught folding two pounds of marijuana into her brownie mix for free distribution to AIDS sufferers. She faced a five-year sentence on felony charges. But all charges against her were dismissed when the local district attorney refused to prosecute. And when Oregon caregiver Sharon Place, arrested in May 1990 for growing 64 plants for free distribution to cancer, MS, and AIDS patients, was convicted of manufacture and possession of marijuana, she faced 18 months—but the judge gave her only two years’ probation and 80 hours of community service.
Whether any of these developments will hasten a rescheduling of marijuana to allow for its prescriptive use is unknown. But there is considerable optimism among medical-marijuana advocates that the election of Bill Clinton will bring a change in federal policy. Clinton’s appointment of Dr. Joycelyn Elders—who favors medical marijuana use under certain conditions—as surgeon general is a hopeful signal. Secretary of Health Donna Shalala’s order to the PHS to look into the Compassionate IND program also bodes well.
But if the decision is made to reopen the program, both Clinton and Shalala will not only have to face political heat from those who applauded the closure of the program. They’ll also have to contend with the bureaucratic question of how to provide medical marijuana to new applicants. This is a problem the PHS never had to contend with, as Compassionate IND access to marijuana was never given to more than 15 people at one time. But with awareness of marijuana’s benefits spreading rapidly through the AIDS, cancer, MS, and paraplegic communities, it is conceivable that tens, and perhaps hundreds, of thousands of people will ask their doctors to apply for the program. Providing the amount of marijuana necessary to meet those needs would require a major effort.
One short-term solution to the problem would be to have the DEA provide confiscated marijuana to the PHS for distribution, after it has been heated to eliminate potentially harmful bacteria or mold. For the long run, the government could simply plant enough to supply citizens needs until licensed private marijuana farms could be established. An alternate to those solutions would be to allow those who need medical marijuana to grow their own, or designate someone to grow it for them.
All of those solutions are political minefields: providing confiscated cannabis raises the question of quality control, since the cannabis would vary widely in potency. Using confiscated marijuana would also lead to the moral quandary of a government encouraging illegal marijuana production to ensure an adequate supply for medicine while imprisoning those who would be the suppliers. And it will be difficult to convince diehard opponents of medical marijuana to back government planting of thousands of acres of cannabis. Licensing private marijuana farms would also bring political heat. And allowing people to grow their own for medical purposes would terrify the police agencies.
But the bureaucratic concerns involved in making marijuana medically available to those who are suffering are only a distraction from the real issue. The question is not how we will solve the problem, but whether the administration is willing to make the effort to solve it. And if so, when?
It remains to be seen in which direction the administration will turn.
“IF IT’S PERCEIVED THAT THE PUBLIC HEALTH SERVICE IS GOING AROUND GIVING MARIJUANA TO PEOPLE, THERE WOULD BE A PERCEPTION THAT THIS STUFF CAN’T BE SO BAD.” —JAMES MASON, DIR. PUBLIC HEALTH SERVICE, JUNE 22, 1991
The U.S. Senate voted, 50-47, on July 22 to confirm President Donald Trump’s nomination of Terrance Cole to be the Drug Enforcement Administration (DEA) Administrator.
Cole, who just last year promoted an article claiming cannabis is linked to higher suicide risks for high schoolers, is now in the driver’s seat of the current cannabis rescheduling hearing process that’s been delayed for six months.
Under an order from DEA Chief Administrative Law Judge John J. Mulrooney II, Cole now has sole discretion on whether the hearing process, to debate the merits of a proposed rule to reclassify cannabis to Schedule III under the Controlled Substances Act, should resume.
Cole told U.S. senators during his April confirmation hearing that “it’ll be one of my first priorities” to review where the DEA is in the administrative process to reschedule cannabis upon being confirmed.
However, Cole provided no promises on the Schedule III proposal that was recommended by former President Joe Biden’s U.S. Department of Health and Human Services and published in the Federal Register after former Attorney General Merrick Garland signed off on a notice of proposed rulemaking. Biden’s DEA never backed the proposal.
Cole told members of the Senate Judiciary Committee that he’d give “the matter careful consideration after consulting with appropriate personnel within the Drug Enforcement Administration, familiarizing myself with the current status of the regulatory process, and reviewing all relevant information.”
Here’s how cannabis industry stakeholders reacted to Cole’s July 22 confirmation vote.
Aaron Smith, Co-Founder and CEO of the National Cannabis Industry Association – (In an Open Letter to Terrance Cole)
“Last year, we were honored to be designated by the DEA as one of the select participants in the agency’s public hearing process for the Notice of Proposed Rulemaking (NPRM) to move cannabis from Schedule I to Schedule III under the Controlled Substances Act.
“NCIA continues to believe that marijuana should not be subject to the Controlled Substances Act (CSA); rather, that marijuana products should be regulated under uniform product safety standards that apply equally to all licensed marijuana businesses and protect consumers across the country, developed under new federal law that recognizes that cannabinoid products cannot be governed under the same regulatory pathways that currently apply to pharmaceutical drugs, food, dietary supplements, alcohol, or tobacco.
“However, our association recognizes that the DEA has only been considering the rescheduling of marijuana. We are eager and ready to work with the DEA and Trump administration to, as you said during your confirmation hearing, ‘listen to the experts’ and ‘follow the science,’ which we are confident will lead to a change in marijuana’s status federally. The rescheduling process under the previous administration was unnecessarily protracted and fraught by allegations of malfeasance within DEA and we look forward to your renewed leadership to expedite this process and fulfill President Trump’s campaign promise to ‘unlock the medical uses of marijuana to a Schedule III drug’ and ultimately ‘implement smart regulations, while providing access for adults, to safe, tested product.’
“As such, we strongly encourage your office to continue advancing the cannabis rescheduling process in a timely and transparent manner. The recent recommendation by the Department of Health and Human Services to reclassify cannabis to Schedule III is grounded in the scientific, medical, and legal standards required by 21 U.S.C. § 811. Rescheduling would help eliminate unnecessary barriers to research, reduce burdens on legitimate businesses operating under state law, and bring federal policy more in line with overwhelming public opinion and decades of state-level reform.
“As DEA considers next steps, we respectfully urge your administration to recognize the importance of collaboration with stakeholders who can offer real-world insights into the public health, enforcement, and operational impacts of federal cannabis policy. NCIA and our members welcome any opportunity to be constructive partners in that effort.” – Aaron Smith
Kyle Sherman, Founder & CEO of Flowhub
“We’re watching the appointment of DEA Administrator Terrence Cole closely. While his background overseeing Virginia’s [Public Safety and Homeland Security] may seem encouraging, questions remain about the political motivations behind his selection. President Trump made clear just last week that this was a Governor Glenn Youngkin-backed appointment and publicly stated he would hold Youngkin accountable if Cole does not deliver. Youngkin, notably, has not been a supporter of the cannabis industry.
“Fortunately, Executive Order 14215, issued by President Trump in February 2025, ensures accountability at the federal level. Section 7 of that order explicitly prohibits agencies and their employees from issuing legal guidance or interpretations that deviate from those of the President and Attorney General. This safeguard exists to prevent political freelancing and keep federal policy aligned with the administration’s commitments.
“If Administrator Cole honors this Executive Order, the will of the public, the President’s promise to unlock safe access to medical cannabis through the reclassification of cannabis to a Schedule III drug, and his own promise to ‘listen to the experts’ and ‘follow the science’ as he testified during his nomination hearing, we’re hopeful he can be an agent of long overdue reform. But we’ll be watching closely.” – Kyle Sherman
Anthony Coniglio, CEO of NewLake Capital Partners
“The conversation around cannabis policy is again clouded by speculation. What we know is limited—but meaningful. Mr. Cole has said cannabis rescheduling will be ‘one of [his] first priorities,’ and that he will rely on science, expert consultation and the framework of the Controlled Substances Act to guide his decision.
“That’s not a political promise—it’s a procedural one. And in today’s regulatory climate, that matters.
“More telling is what Mr. Cole has made unequivocally clear: His focus will be on dismantling fentanyl networks and transnational criminal organizations. That aligns with the DEA’s 2025 National Drug Threat Assessment, which notably downplays cannabis and instead emphasizes synthetic drugs and the organized crime groups behind them. In that context, rescheduling cannabis isn’t just a policy adjustment—it’s a way for the DEA to better distinguish between bad actors and law-abiding, compliance-driven operators.
“Whether Mr. Cole will be a steward of regulatory modernization or a placeholder for the status quo remains to be seen. But the next 100 days offer a chance to turn a long-overdue page. If he leads with science and enforcement clarity—not outdated fears—this could be the start of a smarter, more modern drug policy.” –Anthony Coniglio
Terry Mendez, CEO of Safe Harbor Financial
“The Senate’s advancement of Terrance Cole’s nomination as DEA Administrator is a consequential development for the cannabis industry. With the rescheduling of cannabis under federal law stalled, the incoming DEA leadership will play a defining role in whether that reform moves forward—or remains mired in uncertainty.
“While we welcome Terry Cole’s stated commitment to reviewing the rescheduling proposal, the industry needs more than vague assurances. We need regulatory clarity, fairness, and above all, urgency. The decisions ahead will directly impact the viability of thousands of licensed cannabis operators and the broader financial infrastructure supporting them.
“However, even in the most optimistic scenario where cannabis is rescheduled from Schedule I to Schedule III, we must be clear-eyed about the limitations of that change. Rescheduling does not equate to legalization. It will not eliminate the burdensome compliance regimes that currently deter most large financial institutions from entering the market. Anti-Money Laundering and Bank Secrecy Act requirements will still apply, and the cannabis industry will remain federally criminalized in practice—if not in label.
“Contrary to popular belief, banking services for cannabis businesses are not unavailable today—but they are fragmented, costly, and carried disproportionately by smaller, specialized institutions like Safe Harbor. Rescheduling might offer incremental improvements, but absent updated FinCEN guidance and comprehensive congressional action like the SAFER Banking Act, the financial exclusion of cannabis operators will continue.
“This is a moment to double down on the push for safe banking, tax equity and transparent regulatory treatment. At Safe Harbor, we are committed to ensuring that cannabis businesses—large and small—have access to the financial tools they need to thrive. We urge the new DEA leadership to move swiftly, and Congress to act decisively, so this industry can finally be treated as what it is: legal, regulated, and essential to communities across America.” -Terry Mendez
The Wisdom of Oz: Green Grass, White Powder & Black Sabbath
by Chris Simunek
When you look back at the history of rock’n’roll, it is almost exclusively populated by people from two categories:
Those Who Got Fucked Up, and
Those Who Got Really Fucked Up.
For the latter part of the ’70s and all of the ’80s, Ozzy Osbourne was the Chairman of the Board for category number two. I learned of his legend the way most kids my age did—from pimple-faced geeks in denim jackets with their favorite album painted on the back. The story was always told with the appropriate reverence: He invented heavy metal, he drank a lot, he did a lot of drugs, made some great albums, was kicked out of Black Sabbath for being a loser and then he went solo, bit the head off a bird, bit the head off a bat, pissed on the Alamo, had a guitarist that died in a freak plane crash, went through a period where he looked and dressed a little like Liz Tay lor, and now he is sober and quite successful, albeit a bit shell-shocked.
On the heels of his successful Ozzfest tour, a traveling roadshow that has packaged the likes of Marilyn Manson, Tool, Type-0 Negative and Pantera, Ozzy stunned his fans with the announcement of his reunion with the other members of the original Black Sabbath lineup: guitarist Tony Iommi, bassist Geezer Butler and drummer Bill Ward. It’s something they’d been threatening to do for a decade, but the authentic Sabbath hadn’t played together (aside from a Live Aid appearance) since 1979. On December 5, 1997, they played in their hometown of Birmingham, England, a city of industry that makes Pittsburgh look like Paris, and recorded the show for their new live double-disc set, Reunion.
THE FOLLOWING INTERVIEW GOES TO “II”
Ozzy and Tony Iommi were in New York recently for a Letterman appearance and a meet-and-greet at the new Virgin Megastore in Union Square. When their people contacted HIGH TIMES about a possible interview, I thought it was a prank. I imagined some high school enemy of mine at the other end of the line— “Yeah man, Ozzy wants to hang out and do bong hits with you guys and then Alice Cooper’s gonna drop by with a couple peyote buttons…” Verifying my sources, I found it was true, Ozzy did have something to say to his bonghitting brethren, and was waiting for us in a suite at the St. Regis. Not wanting to undertake such an important mission alone, I invited Rob Braswell, HIGH TIMES’ production director/token metalhead, to join me. What Ozzy and Tony had to say to us we weren’t sure, but we weren’t going to pass up a chance to sit and giggle sycophantically at the feet of our gods.
We arrived early and had a few Berliner weissbiers at the Old King Cole bar to calm our nerves. As we discussed what questions we should ask our favorite air-guitar jamming partners, we both agreed this wasn’t a music interview. If you want to know what Ozzy thinks of the new album or where Tony nicked the riff to “Iron Man,” go read Guitar Player. We wanted tales of rock n roll debauchery, nothing more, nothing less. Ozzy’s people called the bar and informed us that the King of Doom was ready to see us. in the lobby, we were met by a publicist who told us that Ozzy was sick of talking about his indiscretions at American national landmarks and his past cruelties to the animal kingdom. It was implied that a good interviewer might want to steer clear of such subjects.
“Don’t worry,” I told her. ”I just want to talk about drugs.”
Ozzy and Tony were finishing up a previous interview when we walked into their suite. They were both dressed in classic black with large crosses dangling from their necks, sunglasses covering their eyes.
“Are you rolling yet?” Ozzy cracked as we entered.
When you meet Ozzy, it’s kind of like shaking the hand of a man who just came out of a 30-year panic attack. His hands tremble, his voice stutters, but imagine how you’d feel if you’d spent over a quarter-century in a drunken stupor, screaming your ass off in front of a wall of deafening amplifiers, tweaked on enough central-nervous-system stimulants to jump-start Walt Disney’s cryogenically frozen heart. Having heard that Ozzy was completely sober, I asked him if his rolling remark was just a joke.
“Why, you got any?” he inquired.
“Of course,” I said. “You think I’m going to come to this interview emptyhanded?”
“Is there any grown in New York?” he asked.
“Yeah, sure,” I said.
“What I used to do was nip every other leaf so it would grow out instead of up.”
I smiled. Ozzy had given us a genuine grow tip.
“What did you do?” I asked. “Grow it outdoors?”
“Yeah,” Ozzy said with a grin. “But then I got paranoid.”
The word hung there, begging a response.
“Yeah… to coin a phrase. So I’ve got to ask you about Sweet Leaf. Where did that come from?”
“Well, what do you think?” Ozzy laughed. “We used to smoke pounds of the shit, man. We used to buy it by the fuckin’ sackful. We used to be so fucked up all the time. Wake up in the morning, start the day with a spliff and go to bed with it. Yeah, it started to get… I started to get the heebee-jeebees. I was mixing all kinds of other chemicals. Booze, coke, pills…”
“Do you see a difference between pot and other chemicals?”
“Absolutely,” he said, waving his cigarette. “This, for instance, tobacco. I couldn’t smoke as many joints a day as I can this fuckin’ stuff. Gotta legalize pot. I’m all for the legalization of pot, decriminalize it. I don’t smoke it myself, but if anybody wants to smoke it, fine. I got busted for it. We all did.”
“Speaking of busts, what was it like for Black Sabbath to go through Customs in the ’70s?”
“Pretty scary.”
“Did you guys ever have to drop trou?”
“Oh yeah. I remember one time we went from Detroit to Canada through the tunnel. I grabbed one of the guys and asked him, ‘Have we done all the drugs?’ Then I go through my bags and empty them again and, remember them pipes you could get with a fish pump? You got like a fish-tank pump and all these wires and you put the pot in and you just suck on the pipe. They found that.” Ozzy hit his cigarette and chuckled. “Big rubber gloves, the whole nine yards. For fuckin’ smoking pot, man.”
“Do you get more paranoid in the States?”
“I just get paranoid,” he said. “When I do coke I’m like Mr. Paranoia. I’m fucking scared shitless. When you combine it with Demerol and opiates you get real fucked up, you know? You think to get normal, you have to get high. Anything in moderation, but with cocaine I couldn’t.”
“It makes for good VHi documentaries though,” I commented. “You guys in the ’70s had a rep for taking the most amount of time to record records.”
“We were fucked up!” Ozzy laughed at the obvious.
“Which record took the longest?”
“Oh, I don’t know,” Tony answered, not as impressed by Sabbath’s more dubious accomplishments as I was.
“We went to Canada one time, uh…” Ozzy looked at Tony to help him pull the memory out.
“Never Say Die.”
“Never Say Die took fuckin’ forever,” Ozzy said, and the two of them giggled like kids remembering a particularly naughty Halloween prank. “We got this guy coming around giving us bags of cocaine every fuckin’ Wednesday and we’d be like—” Ozzy clenched his face like a coke-freak frozen in action.
“Oh yeah,” Tony said. “When we started out the albums were quick and then…” He shrugged his shoulders, as if there was nothing that could be done about it now.
“With coke,” I wondered, “wouldn’t you record the album fast?”
“You’d do it and then you’d forget what you were doing!” Ozzy said laughing. “We couldn’t turn the fucking tape machine on! We’d turn like pause’ on instead of play/record,’ you know. We’d be playing for fuckin’ twenty-four hours.”
“These neat little bags,” Tony said, reminiscing, “Just chop us another line out! Get another can of beer out the fridge! Roll another joint!” Ozzy shouted. “We used to smoke blocks of hash. Big fuckin’… we used to buy hash by the pound.”
“And coke,” said Tony. “We used to buy these sealed bottles of coke.”
“Government-sealed,” Ozzy added. “We rented this house in Bel Air and we just had these fucking packages up to here—” With his hands Ozzy indicated a pile about the size of a Volkswagen. “It would come in like big gallon-bottles with a spoon on it, covered with a seal of wax. This coke was the best coke that I’ve ever had. I’m lying by the pool one day and I met this guy and I ask him You want to do some coke?’ He goes, No no no.’ I’m whacking this stuff up my nose, it’s a brilliant sunny day, and this guy’s sitting there with one of those reflectors under his chin getting a suntan. I say, What do you do?’ He says, I work for the government.’ Uh… what do you do with the government?’ I work for the drug squad.’ I sez, You’re fucking joking. He shows me his badge. I fuckin’ flipped. I was fuckin’—” Ozzy slammed his fist in his chest like a raging heartbeat. “Flames were coming out of my fingers, man. He says, Oh you’re all right, I’m the guy that got you the coke.’
“We all got fucked up but me and Bill went fuckin’ a little bit further,” Ozzy continued. “Bill ended up in a psychiatric fuckin place. Bill’s antidrug, antidrink, antieverything now. He don’t mince his fucking words either, you know.
With the coke and all these chemicals. 1 got a chemical imbalance in my brain. I’d become really shaky. I have to take Prozac and various medications just to stabilize me.”
“So you never drink, or every once in a while you’ll have something?”
“I don’t drink right now’. Every once in a while is like… I’ve done OK so far, you know’.
I’m not going to say Til never drink again.’ I don’t know. When I’m doing a show’ and I can smell that wonger out in the front, it does tempt me. One thing about the cocaine, though. It used to isolate you and you used to stay in your room paranoid. You buy a bag of white powder and the paranoia soon follows.”
“I’ll never do it again,” said Tony, remembering a promise he once made.
“And when you hear those birds going in the morning tweet-tweet you want to get a fucking machine gun and shoot every bird in sight.
When the day breaks it’s horrible. And what do you do when you wake up? Snnnnnnmmmmfff. Like a fiend, you know.”
“Why is it that so many rock stars crack up?” I asked. “Isn’t it supposed to be the best job in the world?”
“What other job can you imagine where the more fucked up you turn up, the better people think you’re gonna be? Oh fuckin’ Tony’s stoned or Ozzy’s stoned or Bill’s stoned… it’s going to be good fun tonight.’ Too much of anything, eventually you pay a price. If you play now, you pay later, I don’t give a fuck what it is.”
“Is it rough to be sober these days?” I asked, sensing a bit of regret in his voice.
“It sucks,” he replied bluntly. “I don’t like being sober, but say you chopped some lines, I’d go, ’Yeah, I’ll go for it.’ By twelve o’clock I’d be hanging off the fucking building screaming with a bottle of vodka in my hand. Once I start I can’t fucking stop. I gotta go all the way, you know.”
“So what do you do now to fill the gap?”
“Play with my dick,” Ozzy answered with a laugh. “In the ’70s there was a big period of time when I used to drink cheap wine and do ludes. I’d be like fucking jelly and the audience would be like a pond, a fucking oil slick. They were sweaty fuckin’ downed-out fuckin’…” Ozzy trailed off, as if he could still see that placid sea and then asked, “Did you ever try the original Quaaludes?”
The cooler half of Black Sabbath trained their eyes on me and for a moment I felt like a pink, newborn fetus. “No,” I answered with shame. “That’s a little bit before my time.”
“They were fucking wonderful, weren’t they?” Ozzy said and then looked to Tony for confirmation. “I could still get them,” Ozzy offered. “I know somebody who froze ten thousand.”
“Froze them?” I pictured a skinny hipster with sunken cheeks stocking up on 714s so that when the world’s methaqualone supply ran out, he could rise from his bunker and be the Lord of the Lucies.
I was running out of questions and would have to wing a few.
“We were wondering like…” I combed my beery skull for a relevant topic. “Well, since Meatloaf came out with Bat Out of Hell II and Frampton came out with Frampton Comes Alive II, would you ever come out with Volume IV, II?”
“No,” Tony answered as if I should know an artist of his caliber doesn’t repeat himself like that.
“I don’t think so, no,” Ozzy said, pondering the question before a grin split across his face and he let out another tremolo laugh. ” Volume IVII, yeah. Volume IV1/2 * 2… he-he-he.
“We had a question about like, uh… heavymetal fashion in the ’80s.”
“Oh, don’t,” Ozzy started. It was obviously a sore subject.
“What was up with that?”
“I look back at some of those things and I was drinking an enormous amount of booze. Every day I would drink four bottles of Hennessy, a case of Budweiser and as much fucking dope as I could get down my fucking face. As much as I could. I was overdosing on a daily basis.” Ozzy laughed again at the thought of it. Unlike other sober-rockers, he still gets a kick out of his past.
“That’s where the funny clothes came from?” I asked.
“I think that’s where the funny everything came from,” he answered. “We all thought we looked cool. Now we look at ourselves—gay wasn’t even the word. Gay people used to come to us and say, What are you fucking doing, man?’ ” Ozzy pondered for a moment and said, “It’s all part of the crazy world of rock’n’roll.”
I made the mistake of mentioning the time Ozzy put on a dress and redecorated the Alamo and he visibly cringed. It was like asking Achilles to repeat the story about the time he fucked up his heel. He was somewhat appeased when I informed him that this incident was now a highlight of the Alamo tour. At first he didn’t believe me, but I swore to him that a Texan friend had just seen it.
“They should put it in the Guinness Book of World Records.” offered Tony.
“Your own indelible mark upon American history,” I said and a proud, impish smile spread across Ozzy’s face. Our time was running out, so we asked Ozzy to autograph a few records. I handed him my beaten copy of Paranoid. With a quivery hand Ozzy scrawled “Get Stoned” across the gatefold and then signed his name. It was advice from an expert.
Back down at the Old King Cole, Rob and I felt invigorated, like we’d just been to the Rock’n’Roll Doctor and he’d given us a shot of Vitamin Cool.
“He was just like I imagined,” Rob cooed.
“Yeah,” I said, my eyes full of butterflies. That a guy could go through what Ozzy did and still be on top was more than luck, it was damn close to a miracle. When the going got tough, he dressed up in women’s clothing and pissed on national landmarks.
I decided from that point on to try and be more like Ozzy.
He has a message for people like me: If you want a yellow brick road to follow, you have to pause sometimes and paint the stones yourself.
Several reforms to North Dakota’s medical cannabis law are set to take effect August 1, including the sale of low-dose THC edibles and extended timeframes for the validity of medical cannabis cards, the North Dakota Monitor reports.
Edibles now allowed under the medical cannabis program may contain no more than 5 milligrams of THC and no more than 50 milligrams per package. The products can be in the form of a lozenge or a square shape; other foods or beverages are not allowed.
Jake Mittelsteadt, director of retail operations for Pure Dakota Health, told the Monitor that allowing edibles could be a game changer for patients.
“Since day one of this program, the amount of people that joined the program, that come to the state, everybody, especially in the older demographics, their priorities have always been gummies and edibles.” — Mittelsteadt to the Monitor
Under the reforms, patients will also be able to qualify for the program via telehalth rather than just using telehealth services to renew their medical cannabis cards. Medical cannabis cards are also now valid for two years instead of one.
TG joined Ganjapreneur in 2014 as a news writer and began hosting the Ganjapreneur podcast in 2016. He is based in upstate New York, where he also teaches media studies at a local university.
More by TG Branfalt