Medical marijuana is legally available to only nine people nationwide. The Compassionate Investigational New Drug (IND) program which supplies government marijuana to those nine is jointly administered by the Department of Health & Human Services (HHS), the National Institute of Drug Abuse (NIDA) and the Public Health Service (PHS)—which shut down expansion of the program two years ago, claiming that it sent a “bad signal” to the American public. But with the arrival of the Clinton team in Washington, more tolerant winds may be blowing through the corridors of power. Following an order from Secretary of Health Donna Shalala to review the Compassionate IND, rumors have been dying that the program will be opened to new applicants any day.
PHS spokesman Bill Grigg confirmed that meetings regarding the program have occurred—but said they concerned “how to proceed to look at the issue, rather than on whether and when to reopen the program.”
If the Administration does decide to reopen the program, it faces a road riddled with political and bureaucratic land mines. Keeping it shut is similarly unacceptable: people are going blind from glaucoma and suffering needlessly from the “wasting syndrome” associated with AIDS, muscular disorders, and side effects from cancer chemotherapy. Which way will the Administration turn? Difficult to say. But the story of the creation and closure of the Compassionate IND program must be looked at to grasp what is at stake.
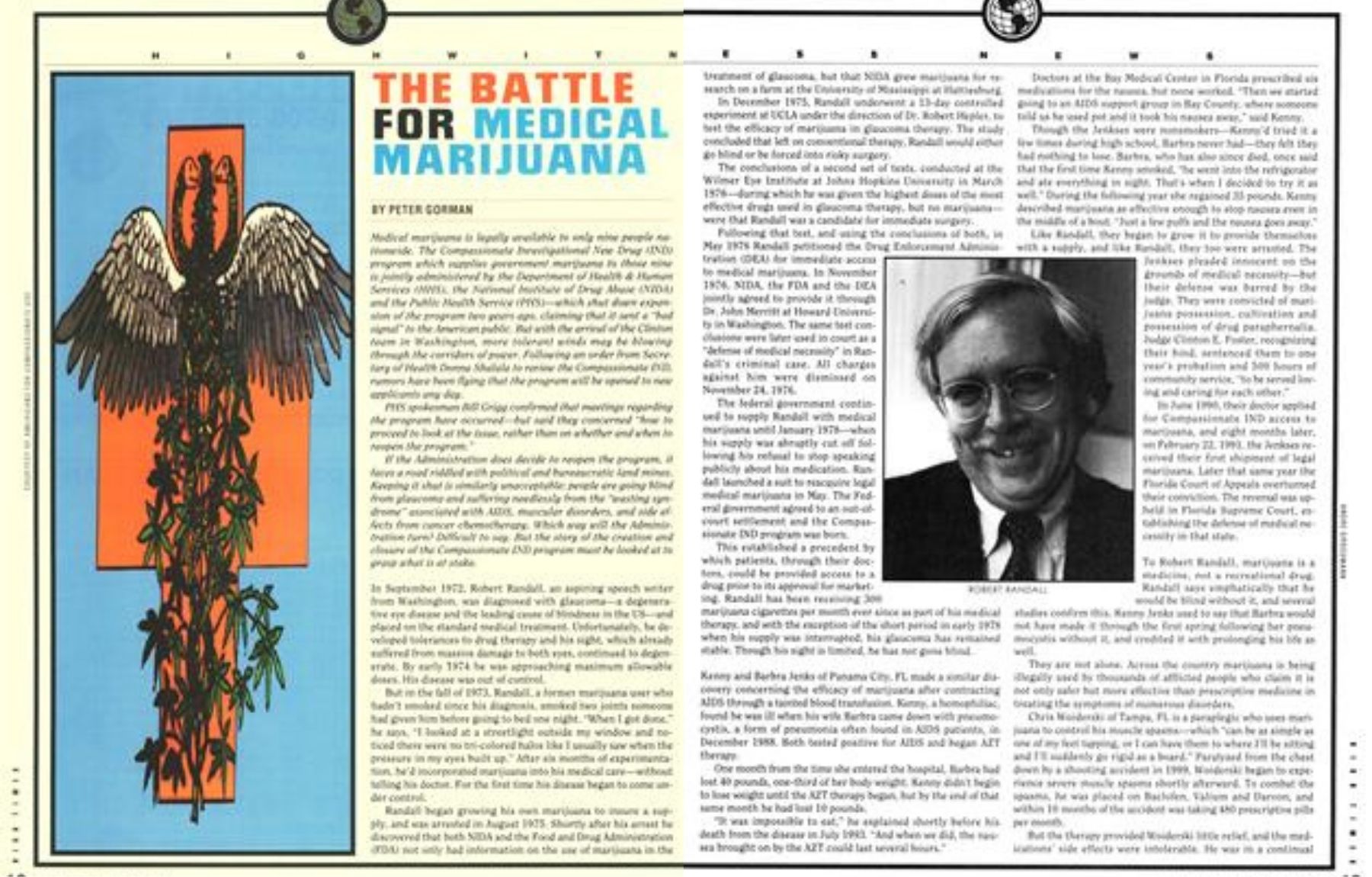
In September 1972, Robert Randall, an aspiring speech writer from Washington, was diagnosed with glaucoma—a degenerative eye disease and the leading cause of blindness in the US—and placed on the standard medical treatment. Unfortunately, he developed tolerances to drug therapy and his sight, which already suffered from massive damage to both eyes, continued to degenerate. By early 1974 he was approaching maximum allowable doses. His disease was out of control.
But in the fall of 1973, Randall, a former marijuana user who hadn’t smoked since his diagnosis, smoked two joints someone had given him before going to bed one night. “When I got done,” he says, “I looked at a streetlight outside my window and noticed there were no tri-colored halos like I usually saw when the pressure in my eyes built up.” After six months of experimentation, he’d incorporated marijuana into his medical care—without telling his doctor. For the first time his disease began to come under control.
Randall began growing his own marijuana to insure a supply, and was arrested in August 1975. Shortly after his arrest he discovered that both NIDA and the Food and Drug Administration (FDA) not only had information on the use of marijuana in the treatment of glaucoma, but that NIDA grew marijuana for research on a farm at the University of Mississippi at Hattiesburg.
In December 1975, Randall underwent a 13-day controlled experiment at UCLA under the direction of Dr. Robert Hepler, to test the efficacy of marijuana in glaucoma therapy. The study concluded that left on conventional therapy, Randall would either go blind or be forced into risky surgery.
The conclusions of a second set of tests, conducted at the Wilmer Eye Institute at Johns Hopkins University in March 1976—during which he was given the highest doses of the most effective drugs used in glaucoma therapy, but no marijuana— were that Randall was a candidate for immediate surgery.
Following that test, and using the conclusions of both, in May 1976, Randall petitioned the Drug Enforcement Administration (DEA) for immediate access to medical marijuana. In November 1976, NIDA, the FDA, and the DEA jointly agreed to provide it through Dr. John Merritt at Howard University in Washington. The same test conclusions were later used in court as a “defense of medical necessity” in Randall’s criminal case. All charges against him were dismissed on November 24, 1976.
The federal government continued to supply Randall with medical marijuana until January 1978—when his supply was abruptly cut off following his refusal to stop speaking publicly about his medication. Randall launched a suit to reacquire legal medical marijuana in May. The Federal government agreed to an out-of-court settlement, and the Compassionate IND program was born.
This established a precedent by which patients, through their doctors, could be provided access to a drug prior to its approval for marketing. Randall has been receiving 300 marijuana cigarettes per month ever since as part of his medical therapy, and with the exception of the short period in early 1978 when his supply was interrupted, his glaucoma has remained stable. Though his sight is limited, he has not gone blind.
Kenny and Barbra Jenks of Panama City, FL, made a similar discovery concerning the efficacy of marijuana after contracting AIDS through a tainted blood transfusion. Kenny, a hemophiliac, found he was ill when his wife Barbra came down with pneumocystis, a form of pneumonia often found in AIDS patients, in December 1988. Both tested positive for AIDS and began AZT therapy.
One month from the time she entered the hospital, Barbra had lost 40 pounds, one-third of her body weight. Kenny didn’t begin to lose weight until the AZT therapy began, but by the end of that same month he had lost 10 pounds.
“It was impossible to eat,” he explained shortly before his death from the disease in July 1993. “And when we did, the nausea brought on by the AZT could last several hours.”
Doctors at the Bay Medical Center in Florida prescribed six medications for the nausea, but none worked. “Then we started going to an AIDS support group in Bay County, where someone told us he used pot and it took his nausea away,” said Kenny.
Though the Jenkses were nonsmokers—Kenny’d tried it a few times during high school, Barbra never had—they felt they had nothing to lose. Barbra, who has also since died, once said that the first time Kenny smoked, “he went into the refrigerator and ate everything in sight. That’s when I decided to try it as well.” During the following year she regained 35 pounds. Kenny described marijuana as effective enough to stop nausea even in the middle of a bout. “Just a few puffs and the nausea goes away.”
Like Randall, they began to grow it to provide themselves with a supply, and like Randall, they too were arrested. The Jenkses pleaded innocent on the grounds of medical necessity—but their defense was barred by the judge. They were convicted of marijuana possession, cultivation, and possession of drug paraphernalia. Judge Clinton E. Foster, recognizing their bind, sentenced them to one year’s probation and 500 hours of community service, “to be served loving and caring for each other.”
In June 1990, their doctor applied for Compassionate IND access to marijuana, and eight months later, on February 22, 1991, the Jenkses received their first shipment of legal marijuana. Later that same year the Florida Court of Appeals overturned their conviction. The reversal was upheld in Florida Supreme Court, establishing the defense of medical necessity in that state.
To Robert Randall, marijuana is a medicine, not a recreational drug. Randall says emphatically that he would be blind without it, and several studies confirm this. Kenny Jenks used to say that Barbra would not have made it through the first spring following her pneumocystis without it, and credited it with prolonging his life as well.
They are not alone. Across the country marijuana is being illegally used by thousands of afflicted people who claim it is not only safer but more effective than prescriptive medicine in treating the symptoms of numerous disorders.
Chris Woiderski of Tampa, FL is a paraplegic who uses marijuana to control his muscle spasms—which “can be as simple as one of my feet tapping, or I can have them to where I’ll be sitting and I’ll suddenly go rigid as a board.” Paralyzed from the chest down by a shooting accident in 1989, Woiderski began to experience severe muscle spasms shortly afterward. To combat the spasms, he was placed on Baclofen, Valium and Darvon, and within 10 months of the accident was taking 480 prescriptive pills per month.
But the therapy provided Woiderski little relief, and the medications’ side effects were intolerable. He was in a continual drugged state which left him incapacitated. He suffered weight loss, insomnia, severe headaches and developed a problem with his left kidney that now requires surgery.
But while undergoing treatment at the Tampa VA hospital, several paralyzed vets told Woiderski they used marijuana to control their muscle spasms. “I’d smoked occasionally, but never since the accident,” he says, “and I was skeptical. So I investigated at the local university’s medical library and found several papers dealing with marijuana’s success with spasms. So I tried it.”
He discovered that half a joint in the morning before his first transfer from bed to the wheelchair controls his spasms for about six hours. Another half a joint during the afternoon controls them for the remainder of the day, and a whole joint before bed “lets me sleep without being tossed around all night.”
Since then, Woiderski has stopped all prescriptive medication, returned to college, and helped organize Paralyzed Americans for Legal Medical Marijuana (PALM).
On November 16, 1990, Woiderski’s neurologist—who wishes to remain anonymous—applied for Compassionate IND access to marijuana. He was approved on February 16, 1991, but has never received a shipment. HHS started to phase out the Compassionate IND program in June 1991, suspending all shipments to 28 recent approvals. On March 4, 1992, the program was officially shut down for all but those 13 persons who were already receiving the government pot. The only official comment made at the time of the program’s suspension came from PHS Director Dr. James Mason. “If it’s perceived that the Public Health Service is going around giving marijuana to folks, there would be a perception that this stuff can’t be so bad,” Mason told the Washington Post on June 22, 1991. “It gives a bad signal.”
Others in the Bush administration disagreed. Shortly before Mason made his comments, Herbert D. Kleber, the deputy national drug control policy director at the Drug Czar’s office, was “touting the program on national television as a ‘compassionate’ option that was available to seriously ill patients,” according to the Washington Post report. On January 31, 1992, the Los Angeles Times reported that Ingrid Kolb, acting deputy director of the Office of Demand Reduction, another post under the Drug Czardom, “said that dozens of patients who would have been eligible for the drug ‘are suffering from great pain— many are dying.’” She recommended that marijuana be given immediately to patients approved for it.
The decision to shut down the Compassionate IND program has placed thousands of medical marijuana users in the position of having to either continue to secure their marijuana illegally or forego the therapy altogether. “I resent being criminalized because the medicine I use for an incurable disease has arbitrarily been made illegal,” says Connie Tillman, an award-winning public-access cable talk-show host, the mother of two and a multiple sclerosis sufferer who says marijuana markedly decreases her muscle spasms. Others, like Fred Cole, agree. Cole, a fishing guide from Washington state, uses marijuana for back spasms resulting from a logging injury and has spent time in jail for growing marijuana for personal medicinal use.
Before the IND program was shut down, the government had implicitly acknowledged marijuana’s utility in treatment of glaucoma, chemotherapy nausea, chronic pain, the AIDS wasting syndrome and spasm disorders. But studies and anecdotal evidence also suggest it is beneficial in treating arthritis, anorexia, head injuries, epilepsy, migraines, PMS, sickle cell anemia, and stress disorders.
But if marijuana is so effective in the symptomatic treatment of these ailments, why is it illegal as a medicine? And why was the IND program shut down?
Marijuana had been popular in a variety of tinctures until the Marijuana Tax Act of 1937 made prescriptive use of the plant obsolete. The 1937 Act was opposed by the American Medical Association’s lobbyist, Dr. William C. Woodward, but the medical industry ultimately acquiesced to the new order.
There were few protests when the 1970 Federal Controlled Substances Act placed marijuana in the Schedule I category, meaning it had no recognized medical value or applications, and could not be used even for experimental purposes.
Shortly after the Compassionate IND program was shut down, Rayford Kytle, a PHS spokesman, was quoted in the April 1, 1992 Journal of the National Cancer Institute as saying that the program was closed because the “National Institute of Health believes there are better and safer treatments than smoked marijuana for controlling chemotherapy-induced nausea, relieving eye pressure caused by glaucoma and stimulating the appetites of patients with HIV-wasting syndrome.” Kytle added that NIH scientists believe the presence of carcinogens in marijuana smoke poses a significant health hazard to AIDS and chemotherapy patients, whose immune systems are impaired. “There was concern that NIDA’s supply could not keep pace with the increasing demand,” said Kytle.
Both Kytle and PHS chief James Mason made it clear that dronabinol—a synthetic derivative of marijuana, marketed under the name Marinol—would continue to be available for chemotherapy-related nausea.
While there have been no reliable reports of marijuana smokers who do not also smoke cigarettes developing either emphysema or lung cancer, studies indicate that heavy cannabis smoking does produce some respiratory system damage. If an alternate method of delivery could be devised— aerosol spray or vaporization are frequently touted possibilities—that damage could be eliminated. But current US laws banning the production of drug paraphernalia prevent experimentation with these methods. And until new delivery systems are available, proponents feel the potential benefits of smoked marijuana outweigh the dangers. They point to more than 2,000 years of historical medicinal marijuana use worldwide with no long-term negative effects.
Many doctors agree. In a 1990 study conducted by researchers Richard Doblin and Dr. Mark Kleiman, a random, anonymous sampling of 2,430 cancer specialists from the American Society for Clinical Oncology showed 48 percent of the respondents answering that they would prescribe marijuana if it were available, and 44 percent admitted they had already recommended illegal marijuana use to at least one patient.
Kytle’s concern over marijuana’s effects on the immune system also appears unfounded. While early studies did indicate that exposure to large amounts of cannabinoids produced alterations in the immune function of lab animals and cells in vitro, no studies on humans confirmed any correlation between marijuana use and impairment of the immune function.
Kytle’s third reason for the program’s closure, concern that federal supply would not keep pace with increasing demand, might be a reason for producing a larger supply—but doesn’t warrant additional comment.
As for Marinol, it is a synthetic form of the primary active constituent of marijuana, delta-9-tetrahydracannabinol, or THC.
While some users find relief through this pill form of THC, many complain that it doesn’t work as well as marijuana, that it takes longer to begin working, and that they prefer the dosage control they have when smoking marijuana. The National Cancer Institute agreed in a 1992 factsheet titled Marijuana for Chemotherapy-Induced Nausea and Vomiting: “Research has shown that the active ingredient THC is more readily and quickly absorbed from marijuana smoke than from an oral preparation of the substance.”
Medical marijuana proponents maintain that those suffering diseases for which there are no acceptable medical alternatives should have their therapy in the hands of physicians rather than the DEA, which controls the Controlled Substances schedule.
Despite the Public Health Service’s refusal to restore the Compassionate IND program, there is increasing evidence of a change in the public’s view of marijuana as medicine. Proposition P, a medical marijuana measure, was put on the ballot in San Francisco in 1991. It passed with an overwhelming 80 percent of the vote. And in 1992, in considerably more conservative Santa Cruz County, a similar ballot initiative gained 77 percent of the vote. Since then, dozens of similar initiatives and propositions have been passed nationally. Additionally, 35 states have endorsed the use of medical marijuana—although none of them are actually distributing cannabis at this time because the federal agencies which control the supply will not provide it. During the early ’80s, state programs in California, Georgia, Michigan, New Mexico, New York and Tennessee provided nearly 800 patients medical marijuana supplied by the National Institute of Drug Abuse, but federal bureaucratic interference and expense led to their closing.
This change in the perception of marijuana as medicine is rooted in a decision by the DEA’s own Administrative Law Judge Francis L. Young, who ruled in the case of Alliance for Cannabis Therapeutics, et al, vs. US Drug Enforcement Administration, in the matter of Marijuana Medical Rescheduling Petition. In his September 1988 determination, Judge Young said: “One must reasonably conclude that there is accepted safety for use of marijuana under medical supervision. To conclude otherwise…would be unreasonable, arbitrary and capricious….”
On the question of whether the marijuana plant, as opposed to synthetics such as Marinol, should be used, Judge Young said: “The cannabis plant considered as a whole has a currently accepted medical use in treatment in the United States…and it may lawfully be transferred from Schedule I to Schedule II.” The rescheduling would have legalized medical marijuana. But the DEA, under the direction of John C. Lawn, refused to act on Judge Young’s decision.
One of the consequences of the DEA’s refusal to reschedule marijuana was that many physicians who accept marijuana’s therapeutic value began to publicly call for the right to prescribe it. On March 17, 1992, the 450-member House of Delegates of the California Medical Association voted to adopt a resolution sponsored by Berkeley psychiatrist Dr. Todd Mikuriya which, while opposing the recreational use of marijuana, stated that “the therapeutic use of cannabinoids…may be appropriate for certain conditions.” More recently, the House of Delegates for the American Medical Student Association, at their 1993 Miami conference, unanimously endorsed marijuana’s rescheduling. And this past August 26, California became the fourth state to pass a resolution urging the White House and Congress to make marijuana prescriptively available.
These changes in public awareness of medical marijuana have been reflected in court decisions as well. In October 1993, a jury acquitted 39-year-old AIDS sufferer Sam Skipper of two counts of felony marijuana cultivation despite his admission that the more than 20 plants found in his California home were his. It was the first such acquittal in US history.
Additionally, the courts have recently taken a more lenient view of caregivers—those who provide marijuana to seriously ill patients. “Brownie” Mary Rathbun, a 70-year-old from San Francisco, was arrested in July 1992 when she was caught folding two pounds of marijuana into her brownie mix for free distribution to AIDS sufferers. She faced a five-year sentence on felony charges. But all charges against her were dismissed when the local district attorney refused to prosecute. And when Oregon caregiver Sharon Place, arrested in May 1990 for growing 64 plants for free distribution to cancer, MS, and AIDS patients, was convicted of manufacture and possession of marijuana, she faced 18 months—but the judge gave her only two years’ probation and 80 hours of community service.
Whether any of these developments will hasten a rescheduling of marijuana to allow for its prescriptive use is unknown. But there is considerable optimism among medical-marijuana advocates that the election of Bill Clinton will bring a change in federal policy. Clinton’s appointment of Dr. Joycelyn Elders—who favors medical marijuana use under certain conditions—as surgeon general is a hopeful signal. Secretary of Health Donna Shalala’s order to the PHS to look into the Compassionate IND program also bodes well.
But if the decision is made to reopen the program, both Clinton and Shalala will not only have to face political heat from those who applauded the closure of the program. They’ll also have to contend with the bureaucratic question of how to provide medical marijuana to new applicants. This is a problem the PHS never had to contend with, as Compassionate IND access to marijuana was never given to more than 15 people at one time. But with awareness of marijuana’s benefits spreading rapidly through the AIDS, cancer, MS, and paraplegic communities, it is conceivable that tens, and perhaps hundreds, of thousands of people will ask their doctors to apply for the program. Providing the amount of marijuana necessary to meet those needs would require a major effort.
One short-term solution to the problem would be to have the DEA provide confiscated marijuana to the PHS for distribution, after it has been heated to eliminate potentially harmful bacteria or mold. For the long run, the government could simply plant enough to supply citizens needs until licensed private marijuana farms could be established. An alternate to those solutions would be to allow those who need medical marijuana to grow their own, or designate someone to grow it for them.
All of those solutions are political minefields: providing confiscated cannabis raises the question of quality control, since the cannabis would vary widely in potency. Using confiscated marijuana would also lead to the moral quandary of a government encouraging illegal marijuana production to ensure an adequate supply for medicine while imprisoning those who would be the suppliers. And it will be difficult to convince diehard opponents of medical marijuana to back government planting of thousands of acres of cannabis. Licensing private marijuana farms would also bring political heat. And allowing people to grow their own for medical purposes would terrify the police agencies.
But the bureaucratic concerns involved in making marijuana medically available to those who are suffering are only a distraction from the real issue. The question is not how we will solve the problem, but whether the administration is willing to make the effort to solve it. And if so, when?
It remains to be seen in which direction the administration will turn.
“IF IT’S PERCEIVED THAT THE PUBLIC HEALTH SERVICE IS GOING AROUND GIVING MARIJUANA TO PEOPLE, THERE WOULD BE A PERCEPTION THAT THIS STUFF CAN’T BE SO BAD.” —JAMES MASON, DIR. PUBLIC HEALTH SERVICE, JUNE 22, 1991
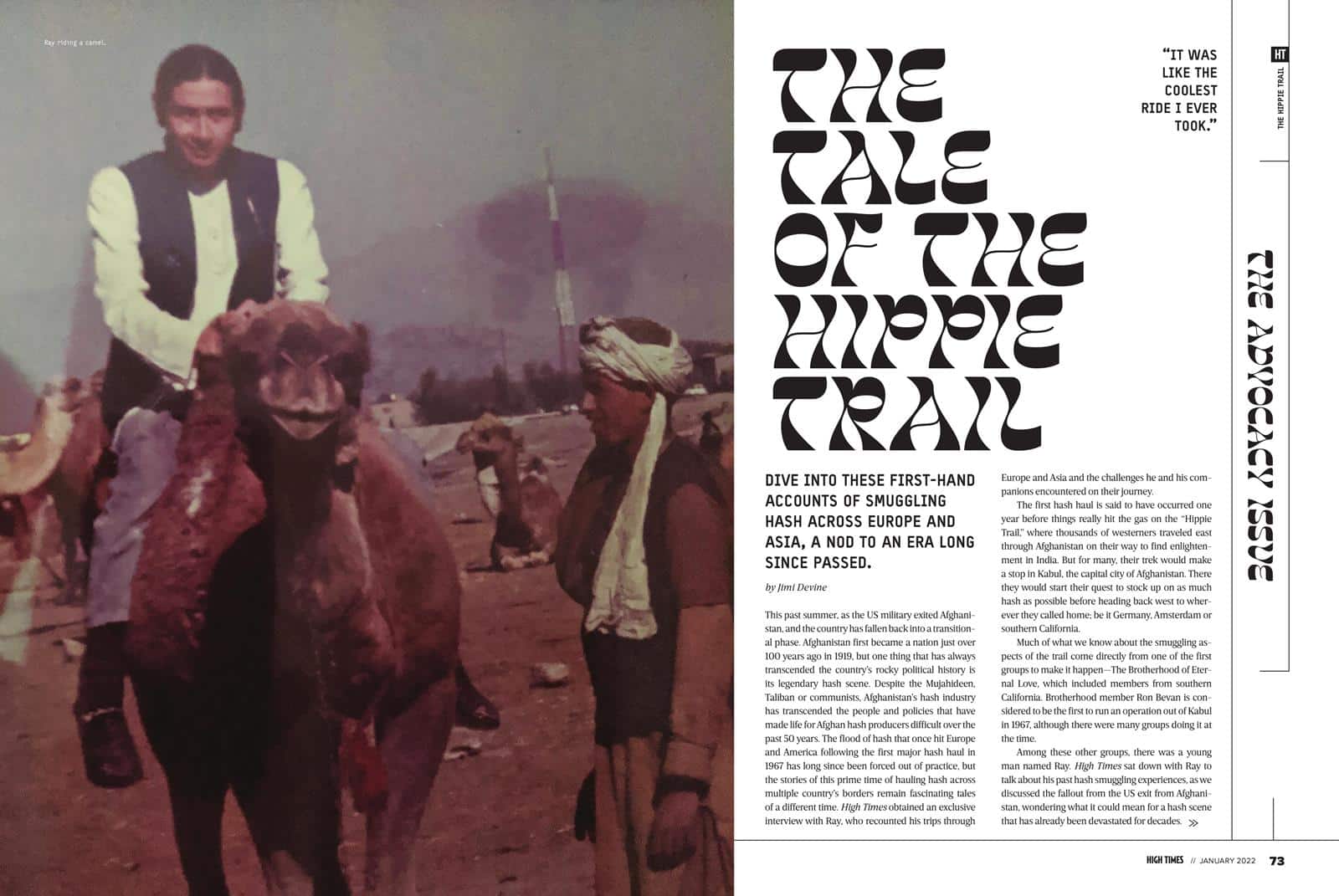
This past summer, as the US military exited Afghanistan, and the country has fallen back into a transitional phase. Afghanistan first became a nation just over 100 years ago in 1919, but one thing that has always transcended the country’s rocky political history is its legendary hash scene. Despite the Mujahideen, Taliban or communists, Afghanistan’s hash industry has transcended the people and policies that have made life for Afghan hash producers difficult over the past 50 years. The flood of hash that once hit Europe and America following the first major hash haul in 1967 has long since been forced out of practice, but the stories of this prime time of hauling hash across multiple country’s borders remain fascinating tales of a different time. High Times obtained an exclusive interview with Ray, who recounted his trips through Europe and Asia and the challenges he and his companions encountered on their journey.
The first hash haul is said to have occurred one year before things really hit the gas on the “Hippie Trail,” where thousands of westerners traveled east through Afghanistan on their way to find enlightenment in India. But for many, their trek would make a stop in Kabul, the capital city of Afghanistan. There they would start their quest to stock up on as much hash as possible before heading back west to wherever they called home; be it Germany, Amsterdam or southern California.
Much of what we know about the smuggling aspects of the trail come directly from one of the first groups to make it happen—The Brotherhood of Eternal Love, which included members from southern California. Brotherhood member Ron Bevan is considered to be the first to run an operation out of Kabul in 1967, although there were many groups doing it at the time.
Among these other groups, there was a young man named Ray. High Times sat down with Ray to talk about his past hash smuggling experiences, as we discussed the fallout from the US exit from Afghanistan, wondering what it could mean for a hash scene that has already been devastated for decades.
Hop In—We’re Going Smuggling
The days before Ray’s first trip to Afghanistan were filled with proper hippie business. “We went to southern Oregon in the late ’60s and for whatever reason out of pure synchronicity a bunch of us from northern California and southern California all ended up in this one house in southern Oregon,” Ray told High Times.
The group decided to take things to the next level and looked to start a commune. They spent some time hunting for a property, but after some hiccups with the search, they regrouped in California in 1968. A lot of the people that originally tossed that idea around remain friends to this day after originally finding each other all those years ago.
Part of that group included some friends who had already been smuggling hash from Afghanistan a year or two before that, and they had just brought back a load. In those days, Ray and his friends were staying in the High Sierras—the perfect place to unload some hash.
Most people associate the “Hippie Trail” with the image of a classic Volkswagen bus and a Hanomag Camper that rolled up to their spot in the same hills that was also very popular with other hash smugglers, such as Darrell. “He came, we unloaded it there, and it took a while. And after he got what he thought was the load amount he goes, ‘Okay, you guys can have the rest.’ And so we picked away at it because it was in the framework,” Ray said, “We had to use all kinds of tools we implement to dig it all out but I think eventually we got like another 10 pounds.”
This would be the first time Ray mentioned the man that he eventually partnered with to make the travel east. “So you know we are quite thrilled to make a connection with him. This is Long Beach, brother, I can give you his name because he’s no longer with us. Well, he had many names, but we knew him as Darrell,” Ray noted with a laugh.
Before connecting with Ray, Darrell had already made two or three trips. He was always a driver, and for good reason. In this critical role, he was the main person who drove from Holland to Kabul and back, through every border. He didn’t even need a map when he was on his runs.
Eventually Darrell shared his next plan with Ray: “Here’s what I want to do next time because I’m gonna have another Honomag, but also I’m going to buy a really nice motorhome,” Darrell told Ray at the time.
The motorhome was called a Revcon. It was the top-of-the-line in 1968 when it was designed. It had an aerodynamic aluminum body, and the 26 rails that ran the length of its frame were a hash smuggler’s dream.
“Very cool, very modern, front wheel drive. And he goes ‘I’m gonna buy this and we’re gonna, this is the vehicle we’re gonna make special rails that go inside the rails and we’ll have little hooks to pull it out,”’ Ray said of Darrell’s original plan.
Ray and Darrell had some friends that were engineers who helped them with building the rails. Eventually they would drive the Revcon across the country from California to New York, shipping it on to Rotterdam, Netherlands.
Darrell asked Ray to tag along for the full run to Afghanistan. “I go, ‘Sure, I’ll go slide and sit shotgun,”’ Ray replied. “It was like the coolest ride I ever took. But we were vegetarian at the time, so we were doing a lot of soups, avocados and carrot juice. We had it all decked out with the Norwalk Press, which is a real good juicing machine. We totally kept our eating habits intact.” Their eating habits would eventually earn them the nickname “The Carrot Juice Boys.”
The group prepped for their journey from Rotterdam after picking up the Revcon. They would make their way through Germany and Austria, then travel through Yugoslavia, Bulgaria, Turkey and Iran before finally reaching the Afghan Border.
That first trip would end up taking a few months, after Ray and Darrell got caught up in eastern Turkey. The Revcon’s front wheel drive engine featured torsion bars in the front, which didn’t pair well with the traffic or potholes they encountered on their journey. They lost control of the Revcon for a second, but were able to come to a stop in the center median. “Eastern Turkey is definitely the sticks, very isolated and very desolate,” Ray said of the breakdown.
When you break down out there, it’s common to surround your vehicle with rocks. They did so before hitchhiking to the closest town. They brought mechanics back to the Revcon, knowing they wouldn’t be able to replace the bar, but could rig something to get the Revcon back to civilization.
They hobbled into Tehran, Iran and messaged home for the part they needed. It wasn’t a fast process. “So we were in Tehran for about a good month, repairing the vehicle, but everything got straightened down,” Ray said, “So we rolled into Afghanistan, probably in late summer of 1970.”
Of Science and Borders
The mission was to obtain a couple hundred pounds of hash and five gallons of hash oil. While other groups had brought hash loads back for about three years before this trip, to the best of The Carrot Juice Boys’ knowledge, they were the first people ever to bring a flash evaporator to Afghanistan. Much of the Revcon was loaded with Everclear for their grand chemistry project.
If the idea of driving across the middle east with a chemistry set seemed weird, the opulence of the Revcon stole everyone’s attention at each border crossing, simplifying getting its contents across various borders in both directions. “I mean, they’ve seen the ‘Hippie Trail’ in the VW Vans, the Honomags, but they’ve never seen anything of this magnitude in this amazing really cool motorhome,” Ray noted on the border crossings. “And of course once we got into Persia we decked it out with Persian carpets and runners and it was looking really cool.”
They were very much playing the part of rich Californians, but they would still be pulled from the line at every border. “The head custom guy would come out and just wanted to go inside and look at it and say ‘oh very nice,”’ Ray said, “It’s just amazing.”
One time, a border agent pulled out their chemistry set and pulled out a beaker. He asked Darrell and the pair what it was. “Glass,” they replied. The border guard looked at it again, nodded in agreement with their take, and put it back in the box.
Iran had some of the toughest border restrictions, but once you entered the country, the group found that it was amongst the most welcoming as they attempted to Westernize before the Shah fell in 1979. Ray emphasized that it was one of the nicest places he’s ever been to, as they spent the month waiting for car parts. “They just want to make sure you’re [not] smuggling weapons or anything, doing nefarious stuff, but all the people there were so nice,” Ray noted of Tehran. “They just were so hospitable and helped us [with] whatever. If we’d go looking for the embassy, [residents] would take us in their car, take us to their home, feed us and then take us to the embassy.”
But with a repaired Revcon, things got a bit rougher as they approached the Afghanistan border. Every hotel featured signs that warned a prison sentence of 10 years in prison for a gram of hash, and life in prison for a kilo. “They try and put the fear in you, but we got some good hash in Turkey,” Ray said with a laugh.
After getting into Afghanistan, the group headed straight for Kabul. They stayed in a fancy neighborhood fitting of rich Californians. From there, they would head to The Solan Hotel, a hotspot for hash enthusiasts and general tourists heading in both directions on the trail.
One of Ray’s favorite things about The Solan Hotel was a space attached to the courtyard where you could park your van and camp near a little park attached to the hotel. There was always an ongoing rotation of Europeans and a few Americans, and it was always a good time.
The locals did their best to keep the hippies and smugglers happy, too. “Afghanis just loved us because we had money and we were very careful about religion,” Ray said. “We were very aware of how they are and how not to trespass or do anything [that] goes counter to them. There’s just some things so you don’t mess with. You don’t eat during the day during Ramadan and walk around chewing food.”
But Ray argued that besides that kind of thing, the religion of Islam was based in hospitality. Over the course of three trips that, in total, took about a year to complete, Ray picked up some language skills. One of the things he noticed immediately was how caring and personal everything was. He noted that a lot of the conversation focused on how the other person was feeling.
Back in their Kabul neighborhood, they rented out a two-story mansion and set up the hash lab. They would do a lot of the extraction work offsite and then bring the crude material back to the flash evaporator in the bathroom to get all the alcohol out. It would take them a couple of months to get the five gallons of hash oil they were shooting for.
“THEY JUST WERE SO HOSPITABLE AND HELPED US [WITH] WHATEVER. IF WE’D GO LOOKING FOR THE EMBASSY, [RESIDENTS] WOULD TAKE US IN THEIR CAR, TAKE US TO THEIR HOME, FEED US AND THEN TAKE US TO THE EMBASSY.”
Unloading the Goods
High Times asked Ray how much hash they needed to make the five gallons. Ray estimated that about 200 kilos were concentrated into the oil. He also noted the unpressed hash made for much better oil, then they hid the rest to stuff in the specialized frames of the Revcon. “The rest we had pressed up and put into the containers, the square tubes, it actually ended up making the hash look like a Hershey bar. We sold most of that in Amsterdam and I’m sure to this day, there are a lot of people there who call it ‘screw hole hash,’” Ray said.
The hash received this name when they put five to seven of the bars together and put a screw through the stack, just to tighten it up before they tossed it down the tube designed to fit into the Revcon’s internal storage system. “It was a precise measurement that we had all the patties pressed,” Ray noted on the precision used to fill each tube with as much product as possible.
As for the oil, that came out pretty great, too. The flash evaporator kept the oil at a reasonable temperature as it sweat off the Everclear used in production. “I mean, it was a black oil. But because of the flash evaporator we didn’t have to heat it in a high temperature, it was in a vacuum, so you got the real essence of really, really good hash,” Ray said. “I don’t know if you’ve had really, really good hash but it’s very floral and very sweet.”
Just like today, in order to make the best oil possible, they had to get their hands on the best material possible. Ray described the process that took them around the country from their upscale Kabul hash lab and base camp. The first connection they ever made was in Kandahar, Afghanistan.
“We used to go to Kandahar, but that was a tough place to be,” Ray noted on the trip. “Kandahar was like going back 1,000 years. I was like ‘Oh my God. That was an ancient town.’ And you couldn’t help but get dysentery just hanging out there for any amount of time. But Kabul was more modern.” In addition to the more modern vibe in Kabul, you could basically get whatever you needed. And in reality, it wasn’t that competitive with other smugglers in town because there was just so much hash to go around.
When it was time to return, the Revcon would leave Afghanistan without Ray. They hired a German woman to play the role of a fancy lady with a fancy motorhome. “We paid her like $10,000 or something. And she was great! She had like a fur coat. I mean, she’d look the part of being wealthy,” Ray said. She was the perfect accessory for a driver who had already completed this trip five times before. The key was the balance of looking like a regular person. Not being an asshole, but also not being too nice, in the hopes of getting waved through borders smoothly.
Ray and Darrell made it to Holland with no problems. The Revcon worked like a charm before being unloaded on a small farm outside Amsterdam. Most of the load would be sold locally.
“But here’s a luggage story for you,” Ray laughed. While the hash moved in Europe, they decided to bring a bunch of the oil back to America. At the time, Ray estimated that the oil was selling for about $10 a milliliter, so a whole liter was worth roughly $10,000 bucks. “We went to a liquor store in Amsterdam and bought Kahlua. Then we’d melt the little seal and stretch it and pull it over the bottle, undo the cap and pour out all the Kahlua and then poured in the hash oil. Then we heated the seal back up and you know back the cap and so it looked sealed, and we’d take two bottles,” Ray said. “So, we go to the airport and we’d go to the duty free and buy another bottle of Kahlua and we traded out the bottle we bought at duty-free. So, we just carried it right across check-in.”
Ray emphasized not to forget the exchange rate. That $10,000 bottle in 1970 would be worth over $70,000 today. He can’t recall how many bottles made it back, the whole five gallons would be worth $1.2 million today.
Adapting the Experience
On Ray’s two trips to Afghanistan, he already had the lay of the land. He flew into Kabul and would buy the hash ahead of time to limit the time spent in the country compared to the marathon road trip and hash oil production of his inaugural adventure.
Ray’s first trip lasted so long he actually overstayed his visa. When he returned for the second run the customs people at the airport noticed it on his passport and gave him a shorter amount of time. After learning his lesson, he got a new passport for the third run. It did the trick, and it was clear sailing at customs. “So, I’d go ahead of time and get there and order up and make sure everything’s ready,” Ray said, “So when the vehicle came through it wasn’t just there, it was like it was going across. It wasn’t there longer than a week or two, which is about the average tourist time somebody might spend there.”
The later runs wouldn’t feature the Revcon. The team moved on to four-wheel drive Suburbans with special compartments in the gas tank that could hold over 100 pounds of gas. The only problem with it was you had to stop a lot more to fuel up, but the trucks did a lot better on the roads than a motorhome.
“But it was pretty safe because to get to it you’d have to take out the whole gas tank and cut into it,” Ray said, “And that was the last time that we did it. We actually hired a professional race driver, who was a dear friend, and he did a good job.”
The gang had a mission of wider psychedelic enlightenment between trips. As they made the runs through the early 1970s, a lot of the resources went into furthering that mission. The freedom Ray and his peers were in search of came with the smuggling and they wanted to make sure to pay it forward. What would start as personal projects for the group would eventually end up in the hands of nonprofits down the line in the form of an unfinished boat. “So the majority of the money that we ever made went on that boat, eventually when the Russians started coming in and put in the puppet government and everything we said, ‘okay, that’s done. We’re not going back there again,”’ Ray said.
Expanding Lore of the First Smuggler
Three years prior to Ray’s first run, Ronnie Bevan of the Brotherhood of Eternal Love would make the first major smuggling run out of Afghanistan. He released the first autobiography of a hash smuggler entitled Brotherhood Hashish: The Story of Ronnie Bevan in 2018.
Many people speak of the “Hippie Trail” as intertwined tales of the many tourists that passed through and a handful of preeminent smugglers like him. High Times asked Bevan to weigh in on that idea. “One thing was there was more than just the two,” Bevan quickly rebutted. “You could get on a bus in London and end up in Kathmandu and there are photos of those people going in 1967 or 1968. The girls have bouffant hairdos and they’re in tight skirts. And then you see him a year later in Kathmandu, and we’re in the hippie clothes and their hair is all down.”
Bevan found that was really the basic motivation of the of the European travelers. Thousands of Europeans made that trip, but very few Americans did, because of the overseas aspect. “We didn’t have the buses. There just weren’t that many. I know, all of the guys that were in Afghanistan smuggling because I was there through several years, and there just weren’t that many,” Bevan said.
Bevan explained that a lot of people in London, or wherever they went from, by the time they got to Nepal all of a sudden they were into the metaphysical side of everything and taking psychedelics. But not everyone. Some people were there for the opposite of self-help. “There also was another large group of people that just did drugs,” Bevan explained, “You could buy heroin, cocaine, you could buy either from the pharmacy in Afghanistan. And consequently, we saw a lot of druggie type people just hanging out. So that’s just another dimension to what you’re talking about.”
Technically, many date the “Hippie Trail” to beginning in 1968, one year after Bevan’s first run. Bevan went on to explain how those increased crowds impacted business. “In the early days nobody got busted for anything, it wasn’t until 1971 that somebody busted [in] one of the vans,” Bevan said.
By 1973, Bevan and his friends had a warrant poster, and he was on the run. That same year Afghanistan’s King Zahir Shah made hash illegal following a $47 million dollar payment from the US government. “Our people had to move into Pakistan to do their work, and it was pretty much destroyed after that. And then it faltered and then a lot of people got busted and especially in those Volkswagens. I think about eight of them, and from that point on, none of them made it they got every one of them but when the Russians came [in] 1979 it was over for sure. That it’s, been over since then.”
A recent article in the South China Morning Post spoke with a cannabis farmer and hash producer outside of Kandahar named Ghulam Ali. Ali noted he hasn’t had any problems since the most recent transition of power, despite concerns that the Taliban would crack down a lot more than the coalition-backed government that fell last summer. “We don’t hear a lot over there. But I think the Taliban is pretty much leaving everything alone,” Bevan replied after reading Ali’s story. “I think what they’re doing is they’re trying to get in there economically.”
It’s also important to remember that hash and Afghanistan have a much longer history than the Taliban does with the nation. “And I think the Taliban probably see that and realize that the people are going to be much happier and much easier to deal with if they let them have their culture,” Bevan argued.
The inhalation of cannabis flower containing THC and CBD provides superior migraine relief compared to a placebo, according to clinical trial data presented at the annual meeting of the American Headache Society.
“This is the first placebo-controlled study in this space. It’s the first real — to me — compelling evidence for the anti-migraine effects of cannabis in humans,” the study’s lead researcher said.
Investigators affiliated with the University of California at San Diego presented the findings. They had previously documented their results in a 2024 preprint paper, concluding, “Vaporized 6% THC+11% CBD cannabis flower was superior to placebo for [migraine] pain relief, pain freedom, and MBS [most bothersome symptom] freedom at 2 hours as well as 24-hour sustained pain freedom and sustained MBS freedom and 48-hour sustained MBS freedom.”
THC/CBD cannabis was also superior to placebo at relieving migraine-related photophobia (light sensitivity) and phonophobia (sound sensitivity).
No serious adverse events were reported.
“Nearly one-third of migraine sufferers have tried cannabis for symptom management, and patients consistently report that it significantly reduces their pain severity and migraine frequency,” NORML’s Deputy Director Paul Armentano said. “These data further affirm patients’ testimonials.”
Survey data indicates that migraine sufferers frequently consume cannabis preparations to mitigate their symptoms and reduce their use of prescription drugs. A 2002 literature review of nine studies involving 5,600 subjects concluded: “Medical marijuana has a significant clinical response by reducing the length and frequency of migraines. … Due to its effectiveness and convenience, medical marijuana therapy may be helpful for patients suffering from migraines.”
The Massachusetts Cannabis Control Commission (CCC) announced Tuesday that the state has surpassed $8 billion in total adult-use sales since the market’s launch.
“The Commission is glad to see the Commonwealth achieve another adult-use cannabis sales milestone, which demonstrates that consumers continue to have confidence in the safety and security of the regulated market.” — CCC Executive Director Travis Ahern, in a press release
Cannabis retailers officially passed the $8 billion mark on June 28, 2025, following a record-breaking start to the year, according to the regulators’ Open Data platform. The development includes record monthly sales this year in January, April, and May, putting Massachusetts on track to beat last year’s annual sales record of $1.64 billion.
“As we anticipate the arrival of Social Consumption businesses – an entirely new license category – in the coming months, we look forward to increasing economic growth for Massachusetts,” Ahern said.
Flower has remained the most popular cannabis product sold by licensed retailers in 2025, responsible for more than $338 million in sales, while vape products ($168.8 million) and cannabis pre-rolls ($116.4 million) are the closest runner-ups.
Meanwhile, the three biggest sales days in Massachusetts (July 2 and April 17-18) either preceded a major holiday or 4/20, which is typically the busiest time of year for cannabis dispensaries.
Based in Portland, Oregon, Graham is Ganjapreneur’s Chief Editor. He has been writing about the legalization landscape since 2012 and has been contributing to Ganjapreneur since our official launch in…
More by Graham Abbott